Cholecystectomy
Key Topics
Introduction
The following information aims to provide information on what the procedure to remove your gallbladder (a laparoscopic cholecystectomy) involves. This is usually performed to treat complications related to gallstones, such as biliary colic, cholecystitis and pancreatitis.
Click here for further information on gallstones and the possible complications they can cause.

Laparoscopic Cholecystectomy
This is usually performed as a day case procedure. You will be asked to attend the pre-admission assessment clinic 1-6 weeks prior to your admission to ensure you are fit for surgery, allowing time for the necessary pre-operative tests, which may include, blood tests, cardiogram (ECG) and a chest x-ray.
You will be admitted on the day of surgery unless there are any medical or technical reasons which would require you to be admitted the day before the operation.
On admission you will be asked to wear TED elasticated stockings to reduce the risk of thrombosis.
The operation is carried out under a general anaesthetic. A telescope the width of a small finger is placed into the abdomen through a small cut at the navel (umbilicus). In order to create space around the organs within the abdomen and provide the surgeon with a clear view it is necessary to introduce carbon dioxide gas to ‘blow up’ the abdomen. Special instruments are passed through three other separate 5-11mm incisions in the abdomen; these enable the surgeon to retract and manipulate the structures within the abdomen and remove the gall bladder. This is all visualized on a video screen by a miniature camera inserted through one of the 4 ‘keyhole’ incisions.
An x-ray (cholangiogram) will usually be performed during the course of the operation to ensure that gallstones have not escaped into the bile ducts: if there is evidence of gallstones within the bile duct (downstream of the gallbladder) they will be removed as well.
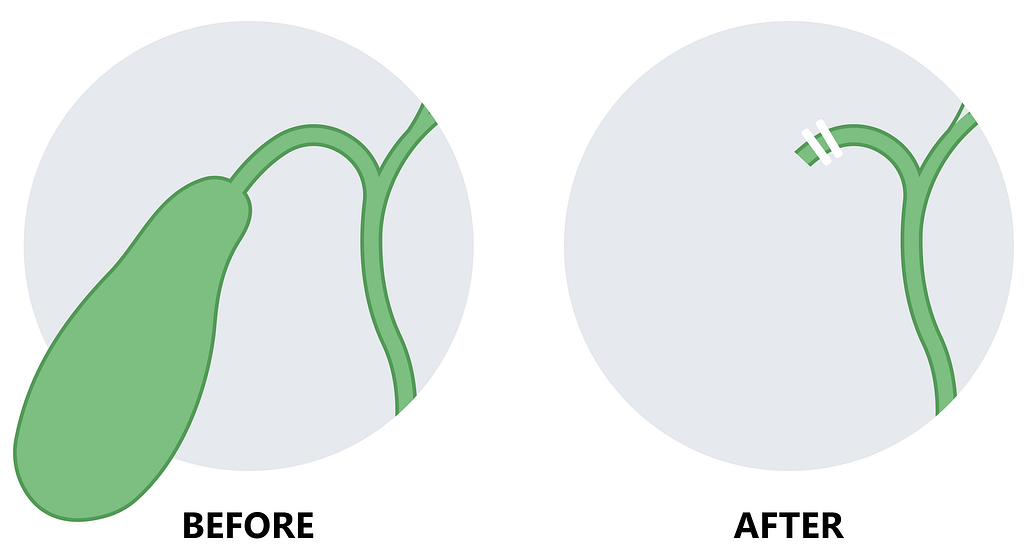
Two clips are applied to the small duct from the gallbladder to the main bile duct and the gallbladder is then removed through the belly button incision.
It may not be possible to access the gall bladder adequately by use of a keyhole incision. It is important to understand that if any difficulties are encountered during keyhole surgery it is in your best interest that your surgeon is free to proceed with an open operation for maximum safety.
What are the risks / complications of surgery?
- The procedure will usually be attempted through a Laparoscopic (keyhole) technique. However, occasionally in 1 to 2% it is not possible to complete the operation using the keyhole technique anda larger incision (an open procedure) may be made. This would entail a longer period of postoperativeconvalescence
- In around 1 in 100 patients, bile may collect in the area where the gall bladder has been removed. This will often necessitate a longer stay in hospital (or coming back into hospital as an emergency) and the insertion of a small drain through the skin in this area or even another operation. This usually presents as pain and temperature about two days after the operation
- Occasionally a small stone may have left the gall bladder and moved into the main bile duct. Sometimes these stones can be removed during the same operation but occasionally a further procedure is required after surgery called an ERCP. This is usually required in about 1 in 100 cases
- There is a very small risk (less than 1 in a 1000) of damage to the main (common) bile duct or the intestines during this procedure. Should this occur further surgical intervention would be necessary. We try to minimise the risk of this as much as possible- the risk is higher in larger individuals where there can be difficulty from fat within the abdomen and in those who have had previous surgery or previous inflammation of the main bile duct.
- Wound infection. Usually the belly button incision as it is prone to collect bacteria. This is quite common in larger individuals. A wound infection can require antibiotic therapy or a small operation to open the wound
- Bleeding after the operation
- Removal of the gallbladder and gallstones is primarily an operation to relieve pain from gallstones and to prevent complications of gallstones such as pancreatitis and cholecystitis (infection of the gall bladder). The operation is unlikely to affect any symptoms that you may have of indigestion, nausea and acid reflux. Occasionally patients may still have persistent pain in the area afterwards despite the operation
These risks/complications will be explained and discussed with you when the surgeon asks you to sign the consent form for the operation.
What should you expect after surgery?
After your operation you may have a drip in your arm giving you fluids initially. However, you will commence fluids as soon as able, if tolerating fluids your drip will be discontinued and you can progress to a light diet.
Abdominal pain/discomfort is to be expected after the operation therefore pain killers may be required for the first 24-48 hours.
Some patients following ‘keyhole’ surgery may experience shoulder tip pain for about a week, this is caused by the abdomen being stretched by carbon dioxide (air), which used to inflate the abdomen at the time of surgery.
If you are feeling sick after your operation, please tell the nurse looking after you, as she will give you an injection to alleviate this.
A tube (drain) may have been inserted, separate from the scar, into the abdomen to prevent the accumulation of blood or bile following surgery; this will be removed after 6-24 hours and the site covered with a dry dressing.
With ‘keyhole’ surgery the small incisions can be closed with steri-strips (paper strips) and covered with a bioclusive dressing: these should remain in place for 5 days. Sometimes the surgeon will use glue- this will dry and flake off after about two weeks.
Because the bioclusive dressing or glue is waterproof you may take a bath or shower.
With ‘open’ surgery if dissolvable stitches are not used then you will need to have your stitches removed 10 days after the operation, you will be informed of the arrangements made for their removal before you are discharged.
The main advantage of ‘keyhole surgery’ is that the period of recovery is far shorter than for an ‘open’ cholecystectomy: the average length of hospital stay is approximately 12 hours with most people going home on the same day as the operation. You will require about 1-2 weeks off work.
For an ‘open’ operation the length of hospital stay is approximately 3 days and the average length of time off work is 4 weeks. Although it must be remembered it may take longer for some individuals to make a full recovery.
If you require a medical certificate for work please ask a member of staff before discharge.
You can resume sexual relations as soon as this feels comfortable.
It is advisable not to drive for at least a week; some people feel they need a little longer. Usually if you can get in and out of the bath without any discomfort and/ or assistance you should be safe to drive. However, please check with your Insurance Company as policies vary with individual companies.
Some swelling or bruising at the wound site(s) is not unusual and there will be some discomfort and tenderness where the incision(s) have been made. In the period following your operation you should seek medical advice if you notice any of the following problems:
- Increased pain, redness, swelling or discharge of the wound(s)
- Persistent bleeding from the wound(s)
- Difficulty in passing urine
- High temperature
- Nausea or vomiting